Part 2
Implant overview.
Hope you made it through the last without falling
asleep/questioning why the hell you would read such a thing. This week’s post
is going to detail a little more about the procedure of placing implants, long
term care and general post implant placement information.
How long
does the whole process take/what do I have to go through.
When answering this question there are various things to be
considered, the main being whether or not the implants are placed and restored
(i.e. placing of the crown or bridge or denture on top of the implant) in
stages vs in one go.
I’m sure you will have all come across those adverts in the
newspaper/the back of certain magazines that offer the operation to place the
implant and then restoration of the implant in a day.
This is incredibly misleading, as it is virtually impossible to
make a denture, crown or bridge to fit on an implant within a day, unless you
have some sort of miracle lab and even then various impressions (moulds) need
to be taken of your implants in order to get the best fit and appearance. If
the dentist is just relying on one impression taken straight after the implants
are placed when there is bleeding, swelling etc then it is highly unlikely that
the crown/bridge/denture is going to fit, look good and work well. Thus if you
went to a decent cowboy dentist they would require at least a couple of visits.
Now this only takes into consideration how it is going to look
immediately. There is some debate within the implant community (a bunch of very
cool people) about the length of time and number of stages that should occur
for the best result.
ADI summarise this nicely.
“For routine cases, from the time of implant placement to the time
of placing the first teeth, treatment times can vary between 6 weeks and 6 months.
The availability of better bone can be used to decrease treatment time, whilst
more time and care must be taken with poorer bone, which can therefore extend
treatment times beyond six months”
They would class routine cases as simple tooth loss
situations i.e. not following cancer treatment or illness, in patients with
suitable bone.
When assessing all patients who are considering implants
there is a basic structure of appointments etc that should be followed if you
want to get the best out of the implants and not destroy your mouth.
Handy subtitle time…
Summary of
stages for routine dental implants
Stage
|
Eh?
|
Other info – if
you’re still with me
|
Diagnosis
|
Your current dentist may be the one who is offering to provide
implants, in which case, they should be familiar with your mouth and
hopefully should have been responsible for doing the groundwork for the time
that you have been seeing them i.e. any fillings, treating gum disease etc.
However different dentists will of course have different opinions and so if
you are going to see an “implant specialist” in another practice, they may
request that your own dentist carries out any dental repairs, filling replacements
or extra courses of gum treatment. Hopefully they wont be pointing out
anything too new and if they do i.e. “good GOD has a bomb gone off in your
mouth”/ “you have RAGING gum disease” then you should perhaps consider
finding a new general dentist.
|
|
Treatment planning
|
Treatment planning involves determination of where the implants are
going to go. Certain things have to be considered at this point:
a. Whether there is enough bone to
support an implant
b. Whether there is enough room to place
an implant and its restoration (e.g. bridge, crown, denture)
c. Whether placing an implant is going
to affect any important things in the mouth i.e. the sinuses/nerves. See some
pictures below for this.
|
a + b
The amount of bone and the amount of space have to be considered in
various different dimensions. There are also different considerations for
each area of the mouth due to the force that teeth take depending on their
position in the jaw. The best way to explain this is with pictures. See
below.
|
1) Vertical dimension: think of it as height of bone/space between the teeth or space between the jaws



Now the above situation is only
for front teeth which generally take a lot less force. Yes you use your natural
teeth to bite into apples etc which technically you can do with implants but
with the amount they cost per piece you’ll probably want to be cutting your
apples up into pieces from now on.
So, for crowns towards the back
of the mouth we need more space because the restorations have to be much
stronger as the back teeth take significant grinding forces. For this reason we
need at least 3-4mm space between
the implant abutment and the opposing teeth.
In the picture below you can
see that the space between the abutment on the implant and the top teeth is
only just 4 mm. In this case this simply is not enough to make a decent white
crown. The reason for this is that the white bit of the crown – the ceramic –
has to be a certain thickness to a) look good and b) be strong enough. At less
than an ideal than an ideal thickness will look like a grey blob and/or break
and fracture as soon as you try and eat something. So for the picture below,
the only option would be to place a full metal crown which can be made much
thinner due to the increased strength of metal over porcelain.
 |
||
The final set of considerations
in terms of measurements is for dentures.
There should be 10–12 mm of vertical space between the implants placed
in either the top or bottom jaw (or in fact both) in order to place good sized
teeth
If a bar is used for the
denture to clip onto – as opposed to simply clipping into the top of the
abutments, then this measurement must allow for a space of 2mm between the gums
and the bar so that it can be effectively cleaned under.

The next measurement to consider is
width of the bone, i.e. between the cheeks/lips and the tongue/palate. Obviously
these measurements all depend on the size of implants the specialist is
intending to use. 3.25 mm diameter implants are the smallest available, according
to dentalcare.com, 6mm width of bone is the minimal thickness into which 3.25
and 4 mm diameter implants can be placed. Larger diameter implants (5 and
6 mm) require at least 7-8mm. Although these measurements are large enough to
accommodate an implant, it means that the implant can only be placed in one
direction as there is limited bone either side of the implant. .


So, miles back, I also mentioned the importance of checking for vital
structures.
1) The sinuses.
These are the bits in your face that
get really painful when you have a cold.

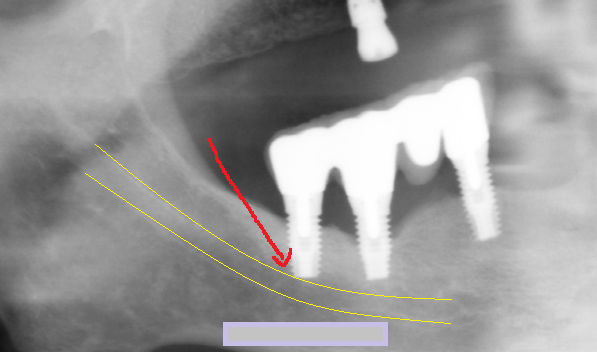
2) Nerves

Once all the above nonsense has been assessed, and
any bone grafts or sinus lifts have been performed (which the specialist can
explain in far greater detail using your own xrays/scans and fun models etc)
then we can get down to the good stuff and actually put the damn implants in.
Stage
|
Eh?
|
Other info – if
you’re still with me
|
Implant Placement
|
Drilling the implant into the bone and the gum
There are 2 different schools of thought as to how exactly this should
go. Of course, the screw part of the implant goes into the bone, but there is
some debate as to whether this screw should then be covered back over and
allowed to heal completely hidden below the gum, OR whether an extra bit (an
abutment) should be placed on top which pokes through into the mouth, and
allow the gum to heal around this.
Time for some more pictures
|
Implant placement is usually followed by a period of healing lasting
from 6 weeks to 6 months.
Stitches are normally removed 7 to 10 days after the implant
placement.
|
Generally,
the process goes a little like this.
1)
Tooth
extracted
a.
At
this point if you had/have a whopping infection like an abscess then the area
will be allowed to heal for a while as placing an implant into infection is
like building a house in sand (and we all know how that song goes)
b.
After
this healing, a space for the implant to go in will need to be made, unlike if
the tooth is just removed and there is a nice space there from where the tooth
was sitting
c.
If
the tooth is just being taken out because of trauma/decay/gum disease then an
implant can be placed into the socket straight away
2)
A
hole for the implant to sit in is made in the bone. Generally there is already
a “hole” from where the tooth was removed but this isn’t a standardised shape
and so the area is shaped to fit the implant perfectly.


3) It
is at this point that the debate starts.
a.
Sometimes
the implant screw is placed and then covered over and the gum is “sealed” with
stitches
b.
Other
times a “healing abutment” is placed on top of the screw which pokes through
the gum. It looks like a small silver button on the gum in the mouth – lots of
fun to scare children with.
i. After either a or b there is a period
of osseointegration a.k.a integration of the implant with the bone of the jaw
before any sort of crown, bridge or denture is placed on them. This allows for
the implant to become more “part” of the jaw than a false object before you start
expecting it to carry the weight of biting force.
ii. This process of osseointegration takes
between 3 and 6 months depending what you read.
iii. During this time you will of course
have a space where the tooth was. If you had coped fine with this space before
seeking an implant then you can carry on with a space, however if you have had
the tooth taken out or it has been knocked out in fact then you may not fancy
walking around with a gap. The only realistic option is a temporary denture
which will replace this missing tooth. Sadly it is a reality that if there is
any period of time of healing then you will need a temporary option to fill the
space and you just have to accept this I’m afraid.
c.
The
implant, abutment and temporary version of whatever the final restoration is
planned to be is placed straight away. The temporary version is not in the
bite, i.e. there is a gap between the teeth so that biting forces are not
applied to the implant while it heals. This of course means that you have a
nicer option than a temporary standard denture but it will not be the final
object and you will have to go back in a few months to have this done.
d.
Of
course the above point is irrelevant if the decision is made to place the
implant, abutment and final
restoration i.e. crown/bridge/denture immediately. Of course this sounds like
the ideal option. Minimal time spent, it’s what they use on those 10 years
younger programmes so it must be good etc however it does not allow any time
for this “osseointegration” before you are expecting a false titanium screw to
stand up to the forces you apply when chewing through an overcooked steak.
Imagine trying to walk on a hip replacement within hours of it being placed.
You just wouldn’t and the same usually applies with dental implants but as with
everything there are differing schools of thought.
Why you SHOULD wait?
|
Why you SHOULDN’T.
|
A study by Adell et al. 1981 conclude that loading i.e. allowing the
implant to take biting forces straight away after placement can interfere
with healing. Ideally, we want bone to form all the way around the implant so
that it becomes almost part of the jaw. If biting forces are applied to the
implant too soon, the implant moves within the jaw (only minimal amounts like
vibrations) meaning that instead of bone forming around the implant, soft
squishy stuff forms instead –like when you pick off a scab too early and this
inevitably will lead the implant to fail.
|
Studies have found that immediate implant loading achieved similar
success rates as those reported in the delayed 2-stage approach therefore,
who cares about all the theory.
|
Covering over the most important bit of the dental implant – the actual
implant bit, allows for safe healing and protection of it from all the
bacteria in the saliva.
|
If the implants are to be placed in the lower jaw, then there is more
chance of success with immediate placing of the final crown/bridge/denture
|
Some research suggests that GENTLE loading of the implant right after
placement actually helps the strength of bone healing around the implant, a
bit like gentle exercise after any operation will help with healing.
|
Stage
|
Eh?
|
Other info – if
you’re still with me
|
Healing
|
As mentioned above, this takes around 3-6 months
|
During this time you will probably be going backwards and forwards to
see whoever placed the implant(s) to
check healing, check how the gum is forming around the implant and to
make any adjustments to temporary dentures etc
|
Restoration
|
This is the placing of the final crown, bridge or denture on top of
the implant.
|
|
Looking after the damn things
|
It is important to again reiterate that dental implants are not
natural teeth. They don’t act in the same way, they don’t fail in the same
way. It is also worth noting that when an implant fails, it is really bad. If
a tooth breaks or has to be taken out, then usually its just the tooth that’s
the problem.
According to Carl Misch, DDS, MDS (lots of letters after his
name so he must be important) “when the implant fails, it
also destroys the bone around the implant” often to the point where the whole
plate of bone in front of the implant (the bit that you can feel under you
gum) is completely lost
Similarly, “if that
implant happens to have been placed on a bone graft, this means that this
particular implant failure could result in insufficient bone to re-implant”
i.e. there’s sod all that can be done if it fails.
|
It is worth mentioning at this point that dental implants don’t last
forever. They have a life span just as hip replacements, boob jobs etc do. If
you look after them well i.e. keep them clean, have regularly checks with
your dentist and hygienist visits, don’t smoke, have ideal medical fitness
then you could be looking at 20 years. HOWEVER during this time you will
likely have to have the crown/bridge/denture on top of the implant modified
as they will get worn or damaged by eating and so on.
|
.
So, in summary,
1)
Don’t smoke
2)
If you have gum disease, don’t even think about asking for an
implant
3)
If you want a quick fix, implants are not for you. Similarly if
the thought of having a scalpel/bone drill coming at you makes you feel
sick/dizzy then implants are not for you
4)
If the thought of having a denture puts the fear into you, then
again, implants are not for you. In 99% of cases you wear a short term denture
while the area of infection after taking the tooth out heals, or while the
implant heals
5)
If you have no bone, you can’t have an implant unless you are
suitable for bone grafting which takes time, effort, money and could
potentially also fail.
6) Go and see a specialist who knows what they're doing and can fix problems if/when they arise
I realise this was probably very hard going on the reading front,
and admittedly it was probably written more for my benefit of learning through
researching but maybe it will help someone!
As always, if you have any questions please feel free to ask. Finally, apologies for the varying fonts used on the pictures, I think I may have been losing the plot as I neared the end.
Stuff I looked at
Gapski R, Wang H-L, Mascarenhas P, Lang NP. Critical review
of immediate implant loading. Clin. Oral
Impl. Res, 14, 2003; 515–527
Adell, R., Lekholm, U., Rockler, B. & Bra˚nemark, P.I.
(1981) A 15-year study of osseointegrated implants in the treatment of the edentulous
jaw. International Journal of Oral Surgery 10: 387–416
Bra˚nemark, P.I., Adell, R., Breine, U., Hansson, B.O.,
Lindstrom, J. & Ohlsson, A 1969
Intra osseous anchorage of dental prosthesis I: Experimental studies
Scandinavian Journal of Plasticand Reconstructive Surgery 3: 81–100.
http://www.drchetan.com/dentalpics/plog-content/images/dental-instruments/dental-implants/dental-implant-14.jpg

{kind=link}
{kind=link}
{kind=link}
{kind=link}